Healthcare
Keeping Services Alive in Remote Areas
In rural Afghanistan, access to health services has always been limited. The Dutch Relief Alliance stepped in to rehabilitate and support primary healthcare centres, integrate essential care services, and retain skilled staff in difficult environments.

Gharaty, Adraskan District, Herat Province
The Gharaty Primary Healthcare Centre is one of a dozen health facilities supported by the Dutch Relief Alliance. The small but well organised centre is located on a windy hilltop.
It provides free primary care to remote communities, maternal and child health services, vaccinations, nutrition support, and medicines to communities who previously had to travel long distances for basic healthcare.
The Dutch Relief Alliance reopened the clinic in February 2025 after it had fallen into disrepair. For many families like Fazal Ahmed's, the Gharaty Primary Healthcare Centre has brought essential care much closer to home.

“I drove 15 kilometres by motor bike to come here, to get some medical care for my child and myself.”
— Fazal Ahmed
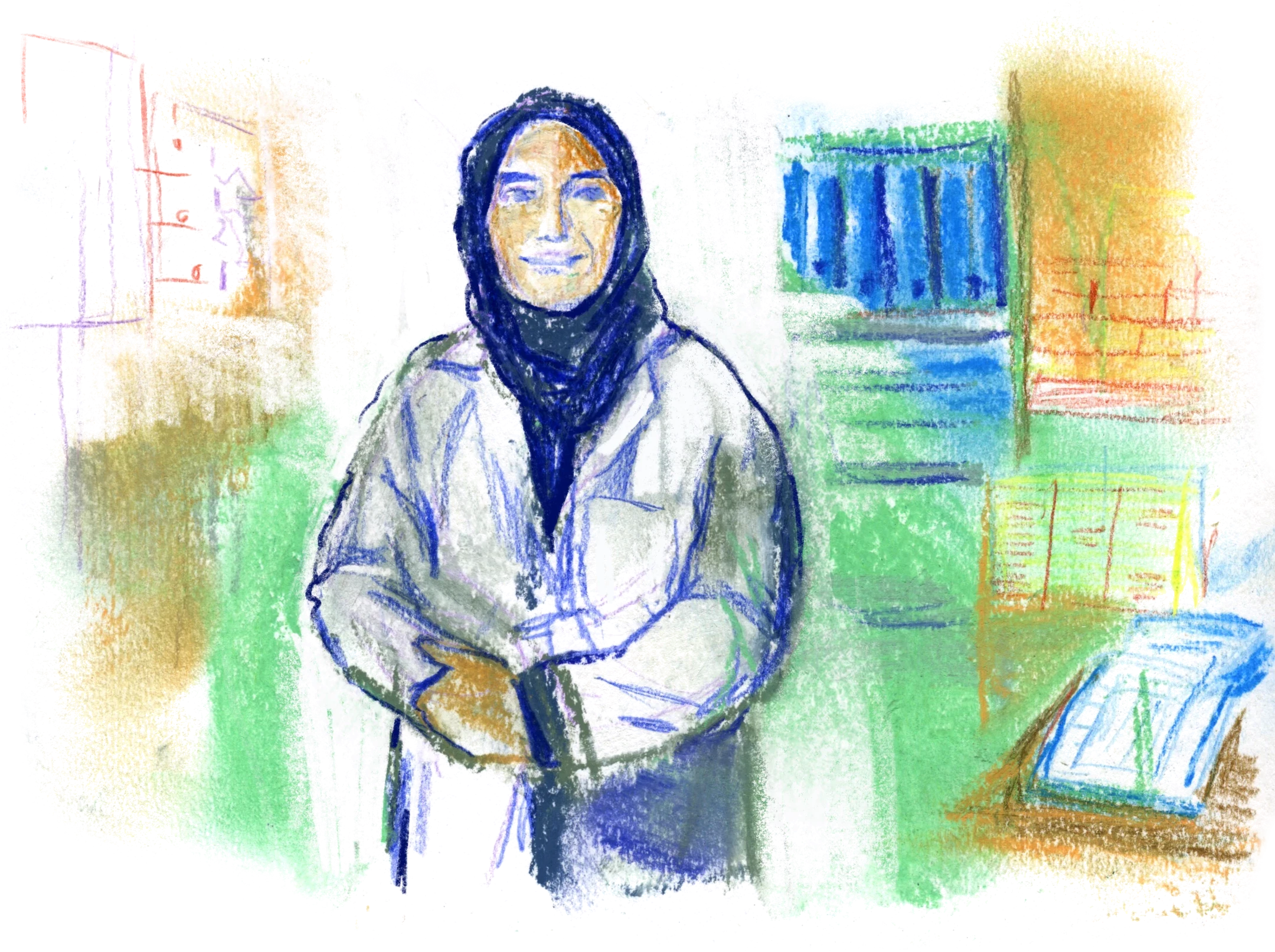
26 year-old Mahbooba Ibrahimi works as a midwife at the Gharaty Primary Healthcare Centre. She provides antenatal, postnatal, and delivery care, family planning, counselling, and health education.

“The biggest challenge women face here is transport. They often arrive too late for consultations or delivery, and sometimes lose their child. That is why reopening this primary healthcare centre has had such an immense impact. Before, people had to travel 25 kilometres further.”
— Mahbooba Ibrahimi

“Maternal and child death rates in this area are going down. It shows the primary healthcare centre really makes a difference. At the same time, the current situation has made it much more difficult for women like me to do our job. When I see women and girls around me forced to give up so much, my will to support them only grows.”
— Mahbooba Ibrahimi
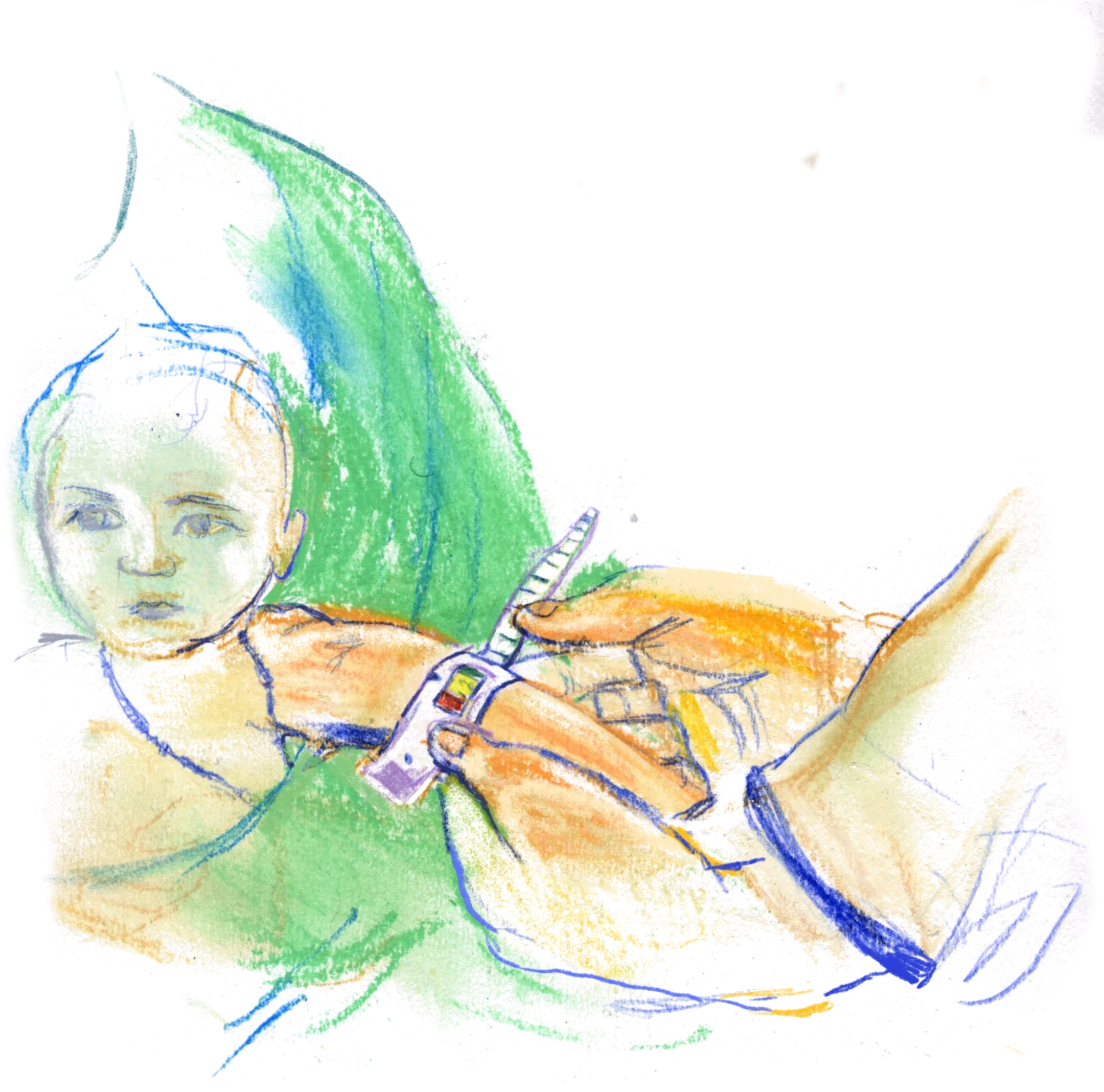
Four months ago, Sima Gull gave birth to her first child, Sumaya, with midwife Mahbooba’s help.


“It was great to receive the care I needed… I am so grateful I did not have to risk a home delivery.”
— Sima Gull
Yekadokan, Kushke Robat Sangi District, Herat Province
The Yekadokan Primary Healthcare Centre in Kushke Robat Sangi, Herat, had been closed for over a year before the Dutch Relief Alliance rehabilitated it with water, toilets, electricity, and solar panels.
Fully funded by the Dutch Relief Alliance, it now provides free care to children, pregnant women, and families across the drought-stricken area. It is located near several villages and hamlets.

Nutritionist Farzana Suri treats under-five children, teaches mothers healthy practices, provides supplements, and supports family planning.
“Child malnutrition is growing here, and it is directly related to climate change. The primary healthcare centre allows us to provide care they otherwise would not get.
Thanks to the Dutch Relief Alliance, I can save lives and reach out to children, mothers, and pregnant women.”
— Farzana Suri


Arezo, 36, is a midwife and mental health nurse. She screens and monitor each pregnant woman and child who comes to her. She teaches mothers how to breastfeed, how to prepare healthy food with what little they have. In cases of severe food insecurity, she provides them with nutritional supplements.
Many women face family violence, forced early marriage, and displacement. The ban on girls’ education leaves teenagers few options, sometimes leading to suicide. Many of her patients are displaced or refugees. They start treatment and then are forced to move again. Monitoring them is very difficult.
“I see young children who do not grow properly because of poverty and drought. Mothers often come to me and say they have no milk and cannot lactate. The standard advice is to watch your diet and eat well… but they have nothing to eat."
— Arezo
The Dutch Relief Alliance provides nutrition support, maternal and child health services and community-based treatments for malaria, diarrhoea, and acute respiratory infections in the health centres.
Besides this, individuals are supported with mental health consultations, as well as awareness sessions on child protection. When a family struggles for food, children often face the highest risks, including child labour or early marriage.
While parents are provided with financial support and business training, youths are involved in Psychological First Aid and protection awareness sessions.

Women appear throughout this response as caregivers, professionals, and entrepreneurs. They are midwives stabilising births, nutritionists preventing malnutrition, farmers growing crops out of dry land, tailors supporting families, and trainees grasping one of the last pathways to learning. Yet their contributions unfold within shrinking space. Health workers describe needing a male companion to travel, which drains income, while daughters are barred from continuing school. And still, perseverance stands out. Women like Mahbooba, Farzana and Arezo continue to serve communities despite personal cost.
“Being able to make a difference is the most rewarding part of my
work.”
— Arezo
Read the next chapter:
Vocational Training